

Effective April 1, 2026, OASIS-E2 introduces targeted updates including the transition to Patient Sex (A0810), refined Transportation (A1255) tracking, and the expansion of Hearing, Vision, and Language assessments to the Resumption of Care (ROC) time point to ensure cross-setting compliance and more accurate patient risk profiles.
Overview
The Centers for Medicare & Medicaid Services (CMS) continues its efforts to streamline data collection and align assessment items across post-acute care settings. Following the implementation of OASIS-E1, CMS has finalized the next iteration of the assessment tool: OASIS-E2.
Scheduled for implementation on April 1, 2026, OASIS-E2 introduces several refinements aimed at improving data accuracy, reducing clinician burden, and aligning with the Home Health Quality Reporting Program (HH QRP). While these changes are considered a minor revision compared to the original shift to OASIS-E, Home Health Agencies (HHAs) must understand these updates to ensure compliance and maintain accurate quality reporting.
This blog reviews the key changes in OASIS-E2 and how your agency can prepare for the transition.
OASIS-E2 Item Changes (Effective April 1, 2026)
The transition from OASIS-E1 to OASIS-E2 involves the removal of specific items, the modification of others to match cross-setting standards, and the expansion of certain items to additional time points. CMS has detailed these adjustments in the Official OASIS-E2 Change Table. Below is a breakdown of the items that have been removed, revised, or added to new assessment time points.
Removal of OASIS Items
CMS is retiring several data elements to streamline documentation and align with updated quality reporting measures:
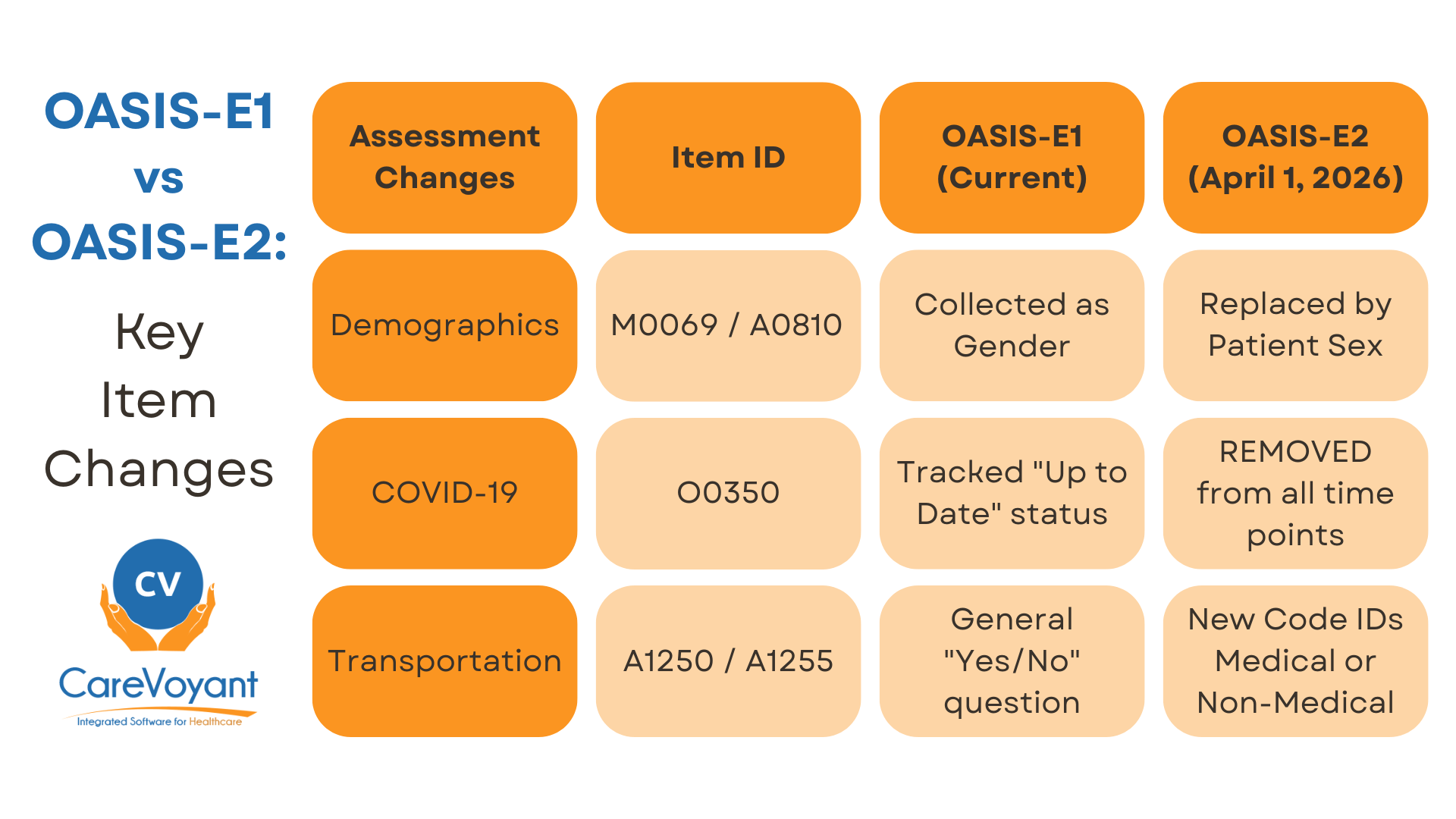
O0350 (Patient’s COVID-19 Vaccination is Up to Date): This item is removed from all assessment time points (Transfer, Death at Home, and Discharge).
A1250 (Transportation): The original general transportation item is retired and replaced by a more detailed version (A1255).
SDOH Items (Living Situation, Food, Utilities): Four Social Determinants of Health items previously finalized in 2025 were removed before implementation to further reduce administrative burden.
Revision of OASIS Items
Existing items have been modified to match the administrative data and language used in other post-acute care settings:
A0810 (Patient’s Sex): Replaces item M0069 (Gender) to align with standardized Medicare administrative data.
A1255 (Transportation): This revised item replaces A1250. It now requires clinicians to specify if a lack of transportation prevented the patient from attending medical appointments or non-medical meetings/work.
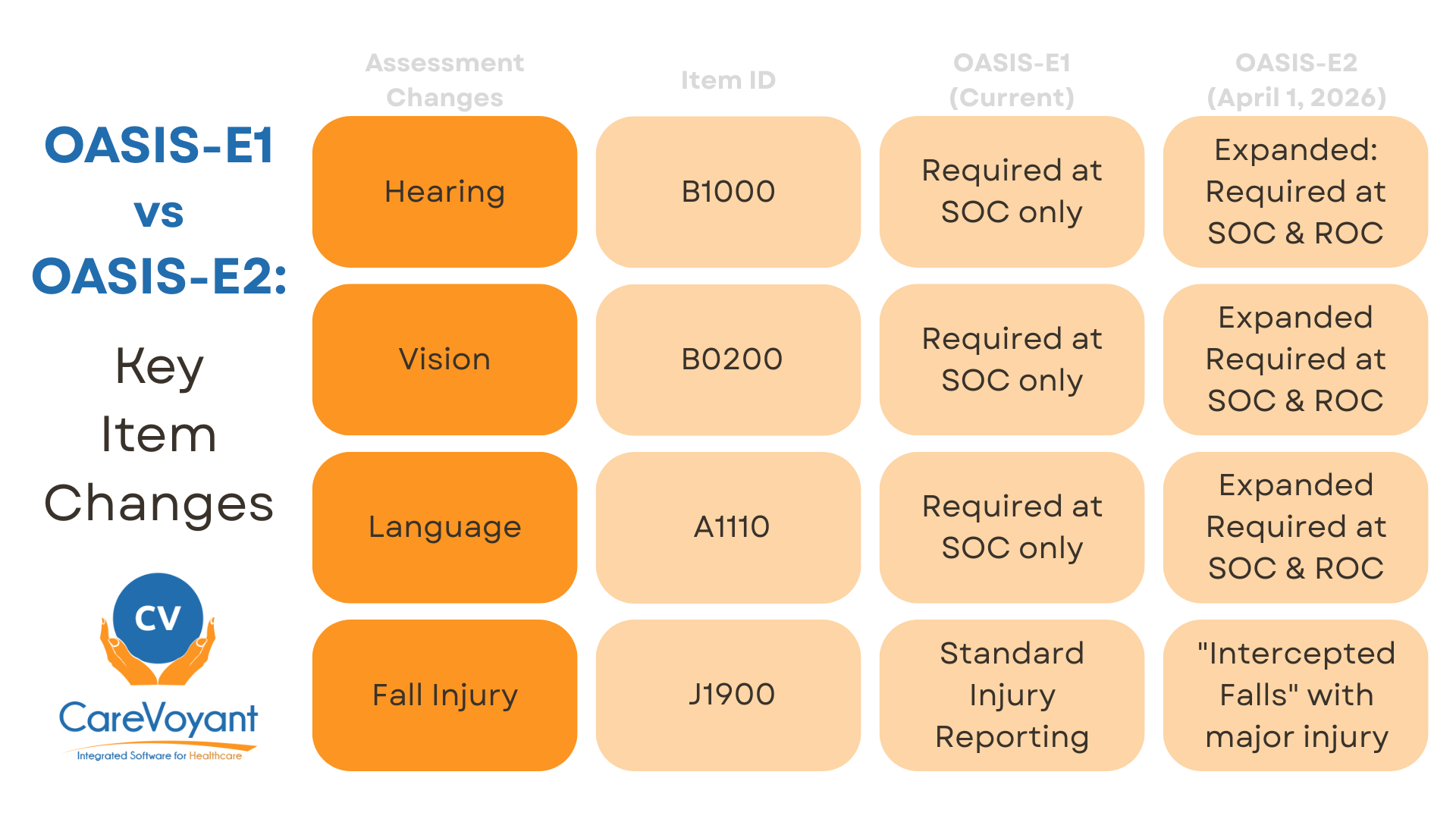
J1900 (Number of Falls): While the item remains, the guidance has been revised to clarify that "intercepted falls" resulting in major injury must be documented more stringently.
Addition of OASIS Items (New Time Points)
To improve continuity of care, several sensory items are now required at the Resumption of Care (ROC) time point:
B1000 (Hearing): Clinicians must now assess the patient's ability to hear during a ROC, a requirement previously reserved for SOC.
B0200 (Vision): Assessment of visual appliances and light/detail seeing is now mandatory at ROC.
A1110 (Language): Preferred language and the need for an interpreter must now be documented upon the patient’s return from an inpatient stay (ROC).
The Impact on Home Health Agencies
While the volume of changes in OASIS-E2 is manageable, the impact on agency operations and clinician workflow should not be overlooked:
All-Payer Requirements: It is important to remember that as of July 1, 2025, OASIS data collection is mandatory for all patients regardless of payer source. OASIS-E2 must be applied to this expanded patient population.
Accuracy in Reporting: Changes to the falls (J-section) guidance mean that clinicians must be more precise in documenting "intercepted falls" to avoid inconsistencies that could trigger audits or impact Star Ratings.
Training Burden: Even minor changes require update training. Agencies should plan for "booster" training sessions to ensure clinicians understand the new A1255 transportation nuances and the addition of ROC requirements for sensory items.
How to Prepare for OASIS-E2
To ensure a smooth transition on April 1, 2026, Home Health Agencies should take the following steps:
Review the Draft Guidance Manual: CMS has released the OASIS-E2 Guidance Manual - Draft. Clinical leadership should review the "Change Table" in Appendix D to identify every specific modification.
Update Clinical Workflows: Adjust your internal assessment protocols to ensure that Hearing, Vision, and Language assessments are consistently performed at the Resumption of Care (ROC) time point.
Coordinate with Your Software Vendor: Your Home Care Software platform is your strongest ally. Ensure your vendor is prepared to implement the OASIS-E2 Data Submission Specifications and provides built-in validation to prevent coding errors.
Role of Home Health Software
The right software platform will play a critical role in helping Home Health Agencies implement OASIS-E2 changes seamlessly. CareVoyant Home Health Software is designed to handle these transitions by providing:
Integrated Documentation: Automatically updating to the newest OASIS versions to ensure clinicians always use the correct forms.
Clinical Decision Support: Built-in alerts and validation rules that flag inconsistencies, such as missing ROC items or incorrect fall reporting.
All-Payer Support: Streamlining the collection of OASIS data for all patients, ensuring compliance with the all-payer mandate and the 2026 OASIS E2 updates.
By proactively preparing for OASIS-E2, agencies can minimize disruptions and continue to focus on delivering high-quality patient care.
OASIS-E2 Frequently Asked Questions
-
The OASIS-E2 implementation date is April 1, 2026. Unlike previous versions that typically launched on January 1st, CMS has scheduled this as an "off-cycle" release. All assessments with a M0090 (Date Assessment Completed) on or after April 1, 2026, must use the E2 version.
-
While OASIS-E1 introduced the all-payer mandate, OASIS-E2 focuses on cross-setting alignment. Key differences include the removal of the COVID-19 vaccination item (O0350), the replacement of M0069 (Gender) with A0810 (Sex), and the addition of sensory items (Hearing, Vision, Language) to the Resumption of Care (ROC) time point.
-
CMS removed O0350 (Patient’s COVID-19 vaccination is up to date) to reduce administrative burden on clinicians. This follows the removal of the corresponding quality measure from the Home Health Quality Reporting Program (HH QRP), as the data was no longer being used for public reporting or reimbursement adjustments.
-
OASIS-E2 replaces M0069 (Gender) with A0810 (Patient’s Sex). This update aligns home health data with other post-acute care settings (like SNFs and IRFs) and matches the administrative standards used by the Social Security Administration and other CMS programs.
-
For the first time, clinicians must now complete assessments for B1000 (Hearing), B0200 (Vision), and A1110 (Language) during a Resumption of Care (ROC). Previously, these were only required at Start of Care (SOC). This ensures that any sensory changes occurring during an inpatient stay are captured immediately upon the patient's return home.
-
Item A1255 replaces the old A1250 transportation item. The new version is more specific, asking how often a lack of transportation has kept the patient from medical appointments or non-medical activities. This is part of the CMS initiative to better track Social Determinants of Health (SDOH).
-
Under the updated guidance for J1800 and J1900, an intercepted fall (where a clinician or caregiver catches the patient) that results in a major injury must be coded as both a fall and an injury. CMS clarified that bone fractures, joint dislocations, and closed head injuries with loss of consciousness qualify as major injuries in this context.
-
Yes. The all-payer mandate that began in 2025 remains in effect. Agencies must use the OASIS-E2 instrument for all skilled patients regardless of whether their payer is Medicare, Medicaid, or a private insurance company.
-
While OASIS-E2 is a minor revision, any change in data collection can impact your Home Health Value-Based Purchasing (HHVBP) scores. Specifically, the more accurate tracking of sensory items at ROC and the refined transportation data will be used in future risk-adjustment models for quality measures.
-
Agencies should focus on three areas:
The ROC Addition: Ensuring clinicians know to check hearing/vision/language at Resumption of Care.
Item Replacement: Training staff on the nuances of the new A1255 Transportation responses.
Documentation: Updating internal QA checklists to reflect the removal of the COVID-19 item to save time during audits.
About CareVoyant
CareVoyant is a leading provider of cloud-based integrated enterprise-scale home health care software that can support all home-based services under ONE Software, ONE Patient, and ONE Employee, making it a Single System of Record. We support all home based services, including Home Care, Private Duty Nursing, Private Duty Non-Medical, Home and Community Based Services (HCBS), Home Health, Pediatric Home Care, and Outpatient Therapy at Home.
CareVoyant functions – Intake, Authorization Management, Scheduling, Clinical with Mobile options, eMAR/eTAR, Electronic Visit Verification (EVV), Billing/AR, Secure Messaging, Notification, Reporting, and Dashboards – streamline workflow, meet regulatory requirements, improve quality of care, optimize reimbursement, improve operational efficiency and agency bottom line.
For more information, please visit CareVoyant.com or call us at 1-888-463-6797.
Request for Information
To learn more about CareVoyant Software and how we improve the operational efficiency of Home Healthcare Agencies, contact us:
