

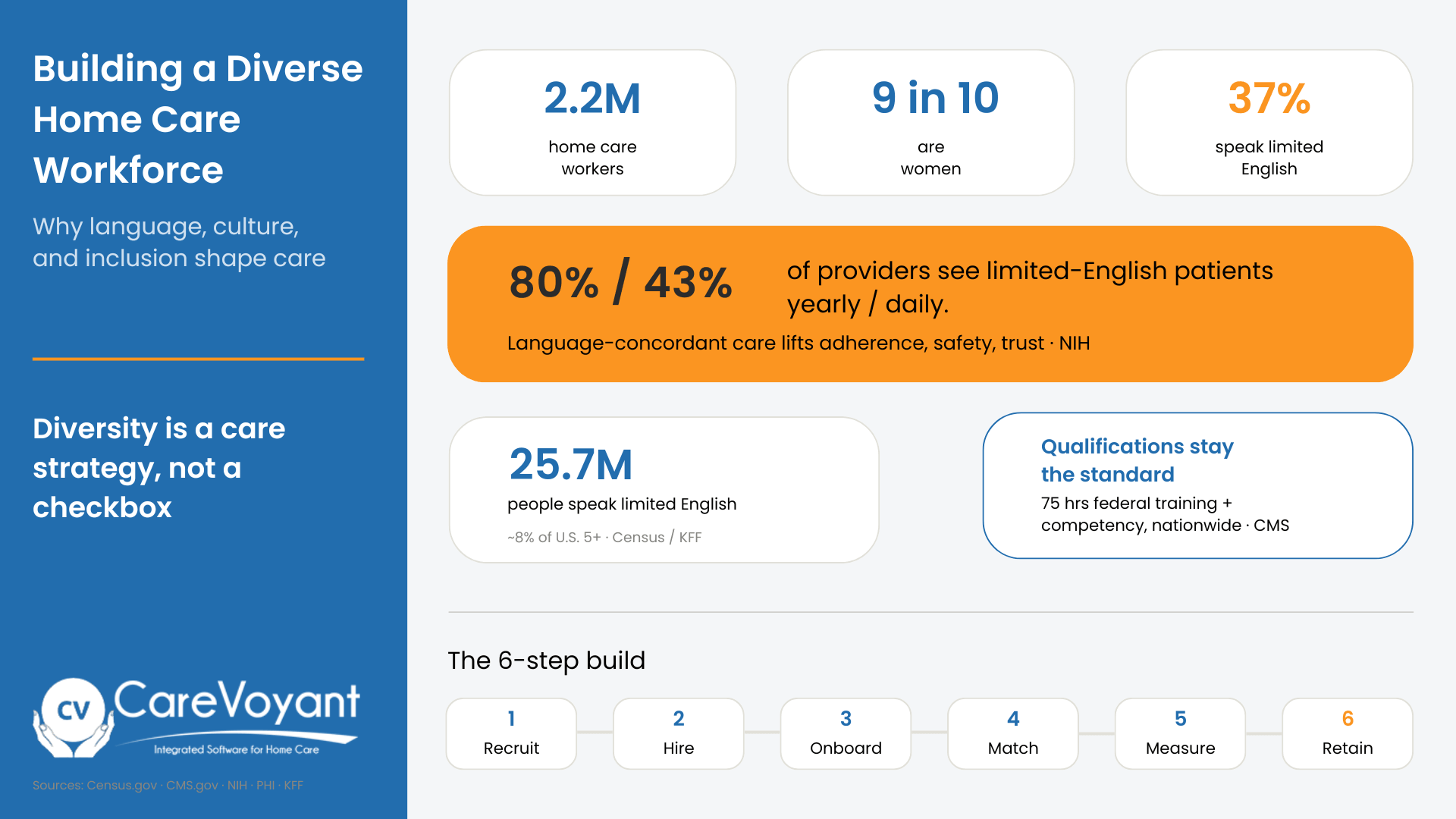
A workforce that matches your patients' languages and cultures improves safety, adherence, and trust while opening referral markets you can't reach otherwise. Roughly 37 percent of home care workers already speak limited English, so the diversity is there to harness. Pair inclusive hiring with better job quality, language-match scheduling, and real tracking, or the effort stalls.
Introduction
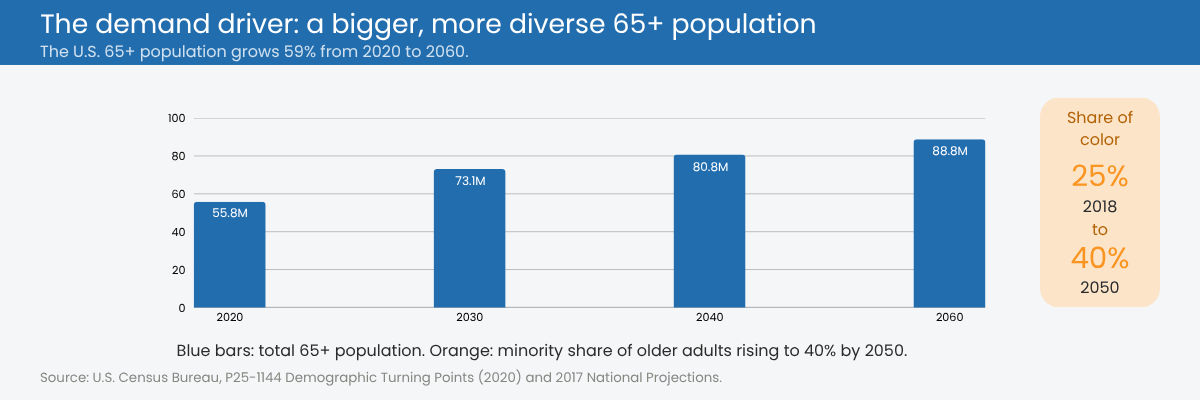
The people receiving home care are getting more diverse faster than the workforce serving them. By 2060, the share of older adults who are Black, Hispanic, Asian, and multiracial will climb sharply, and roughly 25.7 million people in the United States, about 8 percent of everyone age five and older, already speak English less than "very well" (U.S. Census Bureau via KFF). That gap between who needs care and who delivers it is not a soft HR problem. It shapes patient safety, census growth, and whether your agency can compete for referrals in the communities that are growing fastest.
A diverse home care workforce means caregivers who reflect the languages, cultures, and lived experiences of the patients you serve. Building one is now a clinical and competitive necessity, not a values statement you post on a careers page.
Building a diverse home care workforce: the data and the framework at a glance.
Who makes up today's home care workforce?
Before you can widen the pool, it helps to know who is in it. The paid home care workforce sits at about 2.2 million workers, and it has roughly doubled over the past decade as care shifted out of nursing homes and into private residences (PHI). Close to 9 in 10 of these workers are women, and people of color are overrepresented compared with the total U.S. workforce.
Language diversity is already baked in. About 37 percent of home care workers report speaking English "not well" or "not at all," and roughly 87 percent are U.S. citizens, according to PHI's analysis of Census microdata. Foreign-born and immigrant workers are far more likely than average to enter home care, a pattern researchers have tied directly to workforce growth across states (National Institutes of Health).
The point: your workforce probably carries more linguistic and cultural range than your systems currently capture. The question is whether you put it to work on purpose or leave it to chance.
Why it matters #1: serving an increasingly diverse patient population
Demand is the first reason this can't wait. Growing diversity and higher care acuity among older adults will drive home care demand through 2060, and the 65-and-older population is projected to become steadily more diverse over that stretch (PHI).
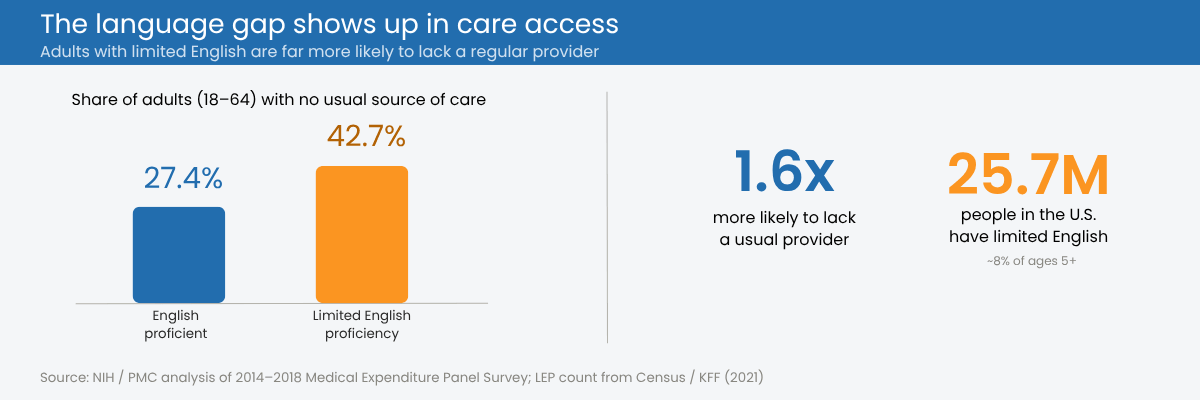
When a caregiver and patient share a language, care instructions land, medications get taken correctly, and safety improves. When they don't, outcomes suffer in measurable ways. Adults with limited English proficiency have worse access to care, higher rates of disability, and lower rates of having a regular provider than English-proficient adults (NIH). Around 80 percent of providers see limited-English patients over the course of a year, and 43 percent see them daily (NIH).
Home care raises the stakes higher than a clinic visit does. Bathing, dressing, feeding, and toileting demand trust and comfort. A patient who can explain what hurts, in their own language, to someone who understands their customs around food, modesty, and family gets better care and feels safer receiving it.
Why it matters #2: language skills as a care and compliance asset
Treat multilingual staff as a coincidence and you leave value on the table. Treat them as a strategic capability and you solve problems your competitors can't.
Federal rules back this up. Section 1557 of the Affordable Care Act and Department of Health and Human Services guidance require meaningful language access for people with limited English proficiency, and the Centers for Medicare & Medicaid Services publishes practical direction on serving these populations (CMS Office of Minority Health). Meeting those obligations with your own bilingual caregivers beats scrambling for a phone interpreter mid-visit.
The care benefits are concrete. Language-concordant caregivers reduce miscommunication, improve visit documentation accuracy, and lower the odds of a preventable readmission. They also cut down on a quiet safety risk: leaning on a patient's child or spouse to interpret medical details, which invites errors and strips privacy. When your scheduling can match a Tagalog-speaking patient with a Tagalog-speaking aide, you are managing risk, not just being considerate.
Why it matters #3: inclusivity as a recruitment and retention engine
The sector is short on workers. The home and community-based services field keeps struggling to attract and keep enough staff to meet demand (NIH / The Gerontologist). Inclusive hiring is one of the few levers that widens the pool instead of fighting over the same shrinking one.
Open your recruiting to bilingual candidates, older workers, career-changers, and people entering healthcare for the first time, and you reach qualified applicants your competitors overlook by habit. Widening the pool never means lowering the standard. Every hire still needs to meet the training, competency, and certification requirements their role and state demand. Retention follows the same logic. Workers who feel culturally seen, supported, and given a path forward stay longer, and turnover is the single biggest cost in this business.
One caution keeps this honest. Diversity efforts fall flat if the job itself stays punishing. Median wages for home health and personal care aides fall below the national median in most Southern states, ranging from about $20,800 in Louisiana to $37,010 in the District of Columbia in 2023 (NIH). Inclusive hiring works when it comes paired with fair pay, training, and real advancement, not as a substitute for them.
The business case: market reach and competitive differentiation
Diversity reads as an ethics topic, but it lands on your income statement. Agencies that can serve limited-English and multicultural communities unlock referral markets that monolingual competitors simply cannot enter.
That reach becomes leverage in Medicaid HCBS contracts, payer networks, and RFPs that increasingly weight health equity. It compounds through reputation, too. In tight-knit cultural communities, one family's good experience travels fast, and referrals follow. Track the payoff where it shows up: referral conversion, census growth, patient satisfaction scores, and star ratings.
Common barriers to building a diverse workforce
Naming the obstacles makes them easier to clear.
The structural ones come first: low wages, thin training budgets, and credentialing hurdles that keep skilled foreign-trained workers from converting qualifications they already hold into roles they're ready for. Then there is bias, often unintentional, baked into how agencies recruit, interview, and even assign shifts. Researchers studying diversity in aged care point to five principles worth training around: awareness of unconscious bias, promotion of inclusion, access and equity, appropriate engagement, and intersectionality (NIH).
Data gaps quietly undercut the rest. Most agencies don't track which languages their caregivers speak or which patients have limited English, so they can't match, measure, or improve. And the pandemic left a mark, pushing women out of the care workforce at a disproportionate rate as caregiving duties collided with paid work (Illinois Department of Public Health).
How to build a diverse home care workforce?
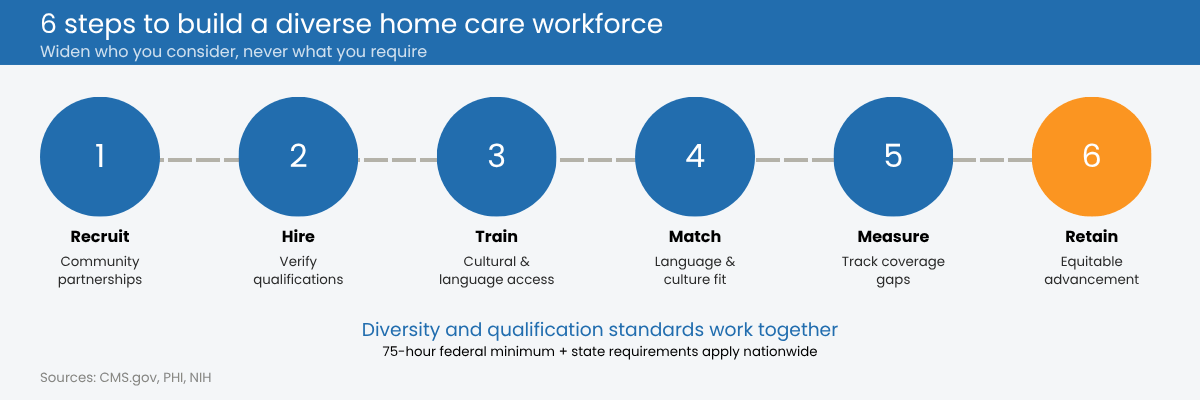
A workable framework moves through six stages.
Recruit through community partnerships, multilingual job postings, and immigrant workforce programs so your pipeline reflects the communities you serve.
Hire with structured, bias-reduced interviews, and verify that every candidate meets the required qualifications for the role. Nationwide, home health aides billing Medicare or Medicaid must complete at least 75 hours of training and pass a competency evaluation under federal CMS rules, and every state layers its own certification, registry, and continuing-education requirements for HHAs, CNAs, and personal care aides on top of that floor. Reward bilingual skills on top of that baseline through a language differential or skill-based pay, never in place of it.
Onboard and train on cultural competency and language access, aligned to CMS guidance, so new hires know how to serve across differences from day one. Use onboarding to close any training or credentialing gaps for candidates whose foreign qualifications don't transfer directly.
Match caregivers to patients by language and cultural fit inside your scheduling process, not as an afterthought.
Measure by capturing caregiver languages and patient language preferences in your agency software, then reporting on coverage gaps.
Retain through equitable advancement, recognition, and wage transparency so the people you worked to recruit actually stay.
How technology makes this practical?
Good intentions need a system behind them. Home care software that stores each caregiver's languages and skills, alongside each patient's language preference, turns diversity from a hope into a field you can filter and act on.
From there, scheduling can match caregivers to patients by language and cultural fit automatically, and reporting can surface diversity and language-access metrics for compliance reviews, payer requirements, and your own quality goals. Platforms built for Private Duty Nursing, Personal Care, HCBS, and Home Health, CareVoyant among them, can hold caregiver skill and language data, drive scheduling around it, and support EVV and documentation so the match you intend is the match that happens.
Diversity is a care strategy, not a checkbox
Three reasons carry this: better patient outcomes, real language access, and a recruiting and retention edge you can't get any other way. None of them is optional, because the demographics are settled. The patients who need home care will keep getting more diverse through 2060, and the agencies that build for that now will be the ones still growing then.
Start with one question this week: does your workforce's language and cultural coverage actually match the patients on your census? If you don't know, that's the first gap to close.
Frequently Asked Questions (FAQs)
-
A diverse workforce lets agencies serve patients across languages and cultures, which improves communication, safety, medication adherence, and trust. It also expands the referral markets an agency can reach and strengthens recruiting in a chronically short-staffed field.
-
Patients with limited English proficiency face worse access to care and poorer outcomes, including higher disability rates and lower odds of having a regular provider. Research on Medical Expenditure Panel Survey data found that 42.7 percent of adults aged 18 to 64 with limited English proficiency lacked a usual source of care, compared with 27.4 percent of English-proficient adults. Language-concordant caregivers reduce miscommunication and preventable readmissions.
-
People of color are overrepresented in home care relative to the total U.S. workforce, and about 37 percent of home care workers report speaking limited English. Immigrant and foreign-born workers are significantly more likely than average to enter the field.
-
Use multilingual job postings, partner with community and immigrant workforce organizations, run structured bias-reduced interviews, and pay for bilingual skills. Pair recruiting with fair wages and advancement so new hires stay.
-
No. Diversity and qualification standards work together. Every hire still needs to meet the training, competency, and certification requirements their role requires. Across the United States, Medicare and Medicaid home health aides must complete at least 75 hours of training and pass a competency evaluation under federal CMS rules, and each state sets additional minimums on top of that. Inclusive hiring widens who you consider, not what you require. Where a strong candidate's foreign credentials don't transfer, onboarding and training close the gap.
-
Section 1557 of the Affordable Care Act and HHS guidance require meaningful language access for people with limited English proficiency, and CMS publishes direction on serving these populations. Requirements vary by program and funding source.
-
When caregivers share a patient's language and cultural background, patients understand their care, feel respected during personal tasks, and build trust, which shows up in higher satisfaction scores and stronger family referrals.
About CareVoyant
CareVoyant is a leading provider of cloud-based integrated enterprise-scale home health care software that can support all home-based services under ONE Software, ONE Patient, and ONE Employee, making it a Single System of Record. We support all home based services, including Home Care, Private Duty Nursing, Private Duty Non-Medical, Home and Community Based Services (HCBS), Home Health, Pediatric Home Care, and Outpatient Therapy at Home.
CareVoyant functions – Intake, Authorization Management, Scheduling, Clinical with Mobile options, eMAR/eTAR, Electronic Visit Verification (EVV), Billing/AR, Secure Messaging, Notification, Reporting, and Dashboards – streamline workflow, meet regulatory requirements, improve quality of care, optimize reimbursement, improve operational efficiency and agency bottom line.
For more information, please visit CareVoyant.com or call us at 1-888-463-6797.
Request for Information
To learn more about CareVoyant Software and how we improve the operational efficiency of Home Healthcare Agencies, contact us:
